2026.04.30 (목) 20:34
2026.04.30 (목) 20:34








 의료공백이 일상인 농촌 주민들 / 사진제공=호남뉴스 |
지역의사 양성법 시행령·시행규칙 제정안 2월 2일까지 입법예고.
지방의료 붕괴를 더 이상 방치할 수 없다는 문제의식 속에서, 정부가 지역의료 인력 확보를 법으로 강제하는 제도를 내놓았다.
의과대학 입학 단계부터 지역 복무를 전제로 의사를 양성하고, 이를 이행하지 않을 경우 의사면허 취소까지 가능하도록 한 강력한 법적 장치가 포함됐다.
보건복지부는 「지역의사 양성 및 지원 등에 관한 법률」에 따른 시행령·시행규칙 제정안을 마련해 2월 2일까지 입법예고에 들어갔다.
이번 제정안은 단순한 장학제도가 아니라, 지방 필수의료 공백을 국가가 직접 관리·통제하겠다는 정책 전환으로 평가된다.
▮ 지역의사 제도, ‘선발–지원–복무–제재’ 전 과정을 법으로 묶다
이번 제도의 핵심은 의사 양성 전 과정이 하나의 계약 구조로 연결된다는 점이다.
① 의대 입학 단계에서 지역의사로 선발
② 재학 기간 동안 국가가 비용 전면 지원
③ 의사 면허 취득 후 최소 10년간 지역 의무복무
④ 불이행 시 강력한 행정·법적 제재
지금까지의 지방 의료 정책이 “지원하되 강제하지 않는 방식”이었다면,
이번 제도는 “지원하는 대신 반드시 지역에 남게 하는 구조”로 방향을 바꿨다.
▮ 복무형·계약형 지역의사… 지역 여건 따라 병행 운영
정부는 지역의사 제도를 복무형과 계약형 두 가지로 나눠 운영한다.
◇ 복무형 지역의사
의과대학 입학 단계에서 지역의사로 선발
재학 기간 동안 등록금·생활비 등 전액 지원
의사 면허 취득 후 10년 이상 지정된 지역 의료기관에서 의무복무
사실상 국가가 직접 양성하는 공공의사 모델에 가깝다.
◇ 계약형 지역의사
이미 면허를 취득한 의사가
지방자치단체 또는 지역 의료기관과 계약을 체결
정해진 기간 동안 필수의료 분야 근무
이는 당장 인력이 부족한 지역에 즉각 투입 가능한 보완 수단으로 활용된다.
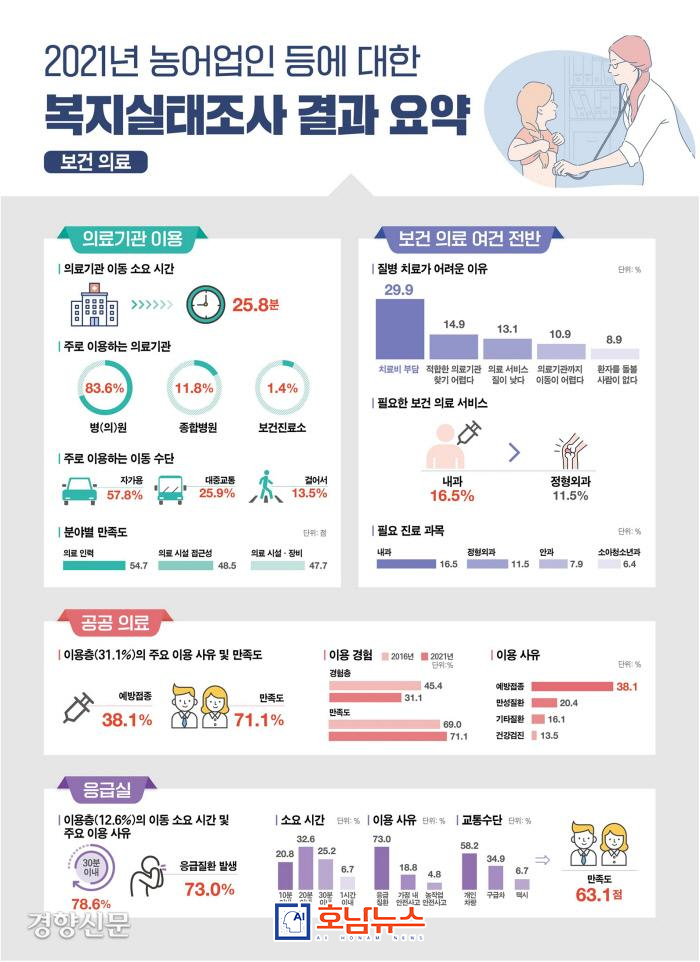 농어업인 복지실태조사 / 사진제공=호남뉴스 |
▮ 지역의사 선발전형, 전국 14개 시·도 32개 의과대학에서 시행
시행령에 따르면 서울을 제외한 14개 시·도, 32개 의과대학이 ‘지역의사 선발전형’을 통해 학생을 선발한다.
선발 인원과 비율은
???? 보건복지부장관이 교육부장관과 협의해 매년 고시한다.
이는 지역별 의료취약도, 인구 감소 속도, 필수의료 붕괴 수준 등을 반영해 지역별·연도별로 선발 규모를 조정하기 위한 장치다.
선발된 학생은 정원 내 특별전형으로 입학하며, 입학과 동시에 지역의사 관리 대상으로 편입된다.
▮ 등록금·교재비·기숙사비·생활비 전면 지원
지역의사로 선발된 학생에게는 의대 재학 기간 동안 실질적 전액 지원이 이뤄진다.
지원 항목은 등록금, 교재비, 기숙사비, 생활비 등으로, 경제적 이유로 학업을 중단하지 않도록 설계됐다.
다만, 이 지원은 무조건적인 장학금이 아니다.
국가와 학생 간의 ‘조건부 계약’ 성격이 분명하다.
▮ 휴학·유급·징계 시 즉시 지원 중단
시행규칙 제정안은 지원 중단 사유를 구체적으로 명시했다.
다음과 같은 경우, 해당 기간 동안 모든 비용 지원은 중단된다.
일반 휴학, 유급, 정학, 징계 처분, 이는 학업 관리와 성실 이행을 담보하기 위한 장치로, 지역의사 제도가 단순한 혜택 수단으로 오용되는 것을 차단하기 위한 조치다.
▮ 의무복무 불이행·반복 징계 시 ‘의사면허 취소’
가장 강력한 조항은 면허 제재 규정이다.
다음에 해당할 경우, 의사면허 취소까지 가능하다.
지역의사가 정당한 사유 없이 의무복무를 이행하지 않은 경우 의사면허 자격정지 처분을 3회 이상 받은 경우 이는 공공재정으로 양성된 의사가 지역을 이탈하거나 의료 윤리를 반복적으로 위반하는 상황을 제도적으로 차단하겠다는 정부의 강한 의지를 반영한다.
▮ “지방의료는 선택이 아니라 국가 책임”
이번 지역의사 제도는 지방의료를 ‘개인의 희생’이나 ‘선의’에 맡기지 않겠다는 선언에 가깝다.
의대 정원 확대 논란과 별개로, 이미 배출되는 의사 인력을 어디에, 어떻게 배치할 것인가에 대한 국가 차원의 첫 구조적 해법이라는 점에서 의미가 크다.
특히 응급실 폐쇄, 분만실 중단, 외과 공백이 일상이 된 전남·강원·경북 등 의료취약 지역에서는 이번 제도가 의료 붕괴를 되돌릴 수 있는 최소한의 안전판이 될 수 있을지 주목하고 있다.
■ 편집자 주
지역의사 제도의 성공 여부는 법 조항이 아니라 “10년을 의무로 버티게 할 것인가”가 아니라 “10년을 일할 수 있는 지역을 함께 만들 수 있는가”에 달려 있다.
의료 인력 정책은 이제 양성의 문제를 넘어, 정착의 문제로 들어섰다.
[Jeonnam = Honam News]
aihnnews@kakao.com
“The State Will Take Responsibility for Gaps in Regional Healthcare”
Ten-Year Mandatory Service for Regional Doctors Institutionalized
Essential Medical Workforce Secured Through Dual Tracks: Service-Based and Contract-Based Models
The government has introduced a system that legally mandates the securing of regional medical personnel, driven by the recognition that the collapse of regional healthcare can no longer be left unattended.
Under the new framework, doctors will be trained from the point of admission to medical school with a prerequisite of regional service. Strong legal measures are included, allowing for the revocation of a medical license if mandatory service obligations are not fulfilled.
The Ministry of Health and Welfare has prepared draft Enforcement Decrees and Enforcement Rules pursuant to the Act on the Training and Support of Regional Doctors, and has opened them for legislative notice until February 2.
This initiative is being evaluated not as a simple scholarship program, but as a fundamental policy shift in which the state directly manages and controls the provision of essential medical services in regional areas.
■ A System That Legally Binds the Entire Process: Selection–Support–Service–Sanctions
The core of this system lies in the fact that the entire process of physician training is structured as a single contractual framework.
Students are selected as regional doctors at the medical school admission stage
The state provides full financial support during enrollment
Upon obtaining a medical license, doctors must serve in designated regions for a minimum of ten years
Failure to comply results in strong administrative and legal sanctions
Where previous regional healthcare policies relied on incentives without enforcement, this system marks a clear shift toward “support in exchange for guaranteed regional service.”
■ Two Tracks for Regional Doctors: Service-Based and Contract-Based Models
The government will operate the regional doctor system through two parallel models, depending on regional circumstances.
◇ Service-Based Regional Doctors
Selected as regional doctors at the time of admission to medical school
Receive full financial support, including tuition and living expenses
Required to serve ten years or more at designated regional medical institutions after licensure
This model closely resembles a state-trained public physician system.
◇ Contract-Based Regional Doctors
Licensed physicians enter into contracts with local governments or regional medical institutions
Serve in essential medical fields for a specified period
This model functions as an immediate supplementary measure for regions facing urgent workforce shortages.
■ Regional Doctor Admissions Implemented at 32 Medical Schools in 14 Provinces
According to the Enforcement Decree, 32 medical schools across 14 provinces, excluding Seoul, will operate a Regional Doctor Admission Track.
The number of students and selection ratios will be
???? announced annually by the Minister of Health and Welfare, in consultation with the Minister of Education.
This mechanism allows the government to adjust intake volumes by region and year, reflecting factors such as medical vulnerability, population decline, and the severity of essential healthcare gaps.
Selected students will be admitted through special in-quota admissions and will be immediately placed under regional doctor management.
■ Full Financial Support: Tuition, Textbooks, Housing, and Living Expenses
Students selected as regional doctors will receive substantive full financial support throughout their medical education.
Covered expenses include:
Tuition
Textbooks
Dormitory fees
Living expenses
The system is designed to ensure that financial hardship does not interrupt medical training.
However, this support is not unconditional; it is clearly defined as a conditional contract between the state and the student.
■ Immediate Suspension of Support in Cases of Leave, Repetition, or Disciplinary Action
The draft Enforcement Rules explicitly specify conditions under which financial support will be suspended.
Support will be halted during periods involving:
General leave of absence
Repeating an academic year
Suspension
Disciplinary action
These provisions are intended to ensure academic discipline and prevent the misuse of the regional doctor system as a mere benefit program.
■ License Revocation for Failure to Serve or Repeated Sanctions
The strongest provision concerns license-related penalties.
A medical license may be revoked if:
A regional doctor fails to fulfill mandatory service obligations without justifiable cause
The doctor receives three or more medical license suspension penalties
This reflects the government’s firm intent to institutionally prevent publicly funded physicians from abandoning regional service or repeatedly violating medical ethics.
■ “Regional Healthcare Is Not a Choice, but a State Responsibility”
This regional doctor system represents a declaration that regional healthcare will no longer depend on individual sacrifice or goodwill.
Separate from debates over expanding medical school quotas, the policy constitutes the first structural, state-led solution addressing where and how existing medical personnel are deployed.
In medically underserved regions such as Jeonnam, Gangwon, and Gyeongbuk, where emergency rooms are closing, delivery wards are disappearing, and surgical departments are shrinking, attention is focused on whether this system can function as a minimum safety net to reverse healthcare collapse.
■ Editor’s Note
The success of the regional doctor system will not be determined by legal clauses alone.
The real question is not whether doctors can be compelled to endure ten years, but whether regions can be made livable enough for doctors to willingly work there for ten years.
Healthcare workforce policy has now moved beyond training alone—it has entered the era of retention and settlement.
 ai호남뉴스 박충배 편집/칼럼/논설 aihnnewsr@kakao.com
ai호남뉴스 박충배 편집/칼럼/논설 aihnnewsr@kakao.com